Regular dental visits are crucial
for maintaining optimal oral health for our senior population. Most of our
senior population often struggle with dental care due to retirement age which
therefore, means no dental insurance. Reduced income means that oral health is
no longer a priority despite the importance of it due to fulling other basic
needs.
There are a few programs in Ottawa to help seniors who do not have dental insurance to meet their oral health need. Below are some of the programs that are available:
In
the community, there are multiple locations that will do free screenings and
include a fluoride varnish application along with some dental education (Ottawa
Public Health, n.d.). Some locations may even offer a free denture cleaning.
The Ottawa Public Health has a monthly calendar that can be used by using the
advanced search button and typing in “dental” (Ottawa Public Health, n.d.).
After doing so, a few locations that offer free screenings will show. The
calendar can be accessed at: https://calendars.ottawapublichealth.ca/all/month
There are some denture benefits that can be offered to seniors. The “Essential Health and Social Supports” is for those with low-income; this program provides those in needs for health support (Ottawa, n.d.). Call 3-1-1 to apply for this program (Ottawa Public Health, n.d.). If the application gets approved, an Ottawa Public Health Clinic will offer a denture assessment.
City Dental Clinics:
40 Cobourg Street (Le Patro). Tel: 613-580-9633 (Ottawa Public Health, n.d.)
400-1580 Merivale Road. Tel: 613-580-9631 (Ottawa Public Health, n.d.)
Algonquin College Dental Clinic offers a full dental health assessment which includes up to four x-rays, teeth cleaning, tooth polishing, fluoride treatment, oral health education and nutritional counselling for $45 (Algonquin College, n.d.). The clinic chargers according to the “degree of difficult” and the amount of build up on teeth. This program is a cheaper alternative route for seniors to get a thorough preventive oral care.
It is important to realize how important preventive oral care is for seniors. Not only does it ensure that they have optimal oral health but also increase their quality of life. These programs are available to those seniors who do not have dental insurance and have low income. This ensures that our senior population can still receive the oral care they require.
Proper
oral care for every individual including dependent seniors seems pretty obvious
as part of their daily routine, but what if dependent seniors with lack of
dexterity cannot perform oral care properly and efficiently?
Lack
of dexterity can come alongside a disability. This can be caused by tremors and
the inability to latch on to a device/material (Oral care for dependent seniors, 2019). The dexterity level
should be assessed each continual care to monitor for not only early disease
stages, but also how the client is adapting to using a device (Oral care for dependent seniors, 2019). During the client
assessment phase during their routine dental visits, the dental hygienist (as
well as their caregivers) can assess for their clients’ (Darby and Walsh, 2014):
Range of motion – The client (if able to) is reaching for their oral cavity with their arms and hands. This can determine the length the device needs to be depending on the client’s ability to reach the mouth (Darby and Walsh, 2014).
(Utensil Holder, n.d.)
Grip strength – Some dependent seniors with a disability, such as those with arthritis or neuromuscular disorders, may have difficulty holding certain devices because of how narrow or small they may be. Their grip strength is assessed by having the client hold on to various size of devices. This can also be done by having the hygienist (or caregiver) grip the clients’ hands gently and ask them to squeeze with as much force as possible for 1 minute – this will help determine the strength needed to be able to latch on to the device for a given time that they present with. If they are unable to hold for 1 minute, a universal cuff (such as a Velcro strap) may be recommended in order to hold the device for the needed amount of time (Darby and Walsh, 2014).
Skill level – The clients are observed by the hygienist or caregiver on how they are self-performing oral care for their own oral cavity. During this step, the ones observing will be able to assess any areas that are unable to be reached or are being missed and if they are brushing the tongue (Darby and Walsh, 2014).
For
those dependent seniors with limited dexterity, there are a number of oral self-care
aids that are available/recommended if needed. These devices may be motivating
for the clients to try on their own or with the help of their caregivers (Darby
and Walsh, 2014):
(Don’t Let Hand Pain Prevent Proper Dental Hygiene, 2017)
Plastic rulers and rods – attached to the
toothbrushes and floss holders with heavy electrical tape to avoid from coming
apart (Darby and Walsh, 2014).
A toothbrush with a compact head size to
better fit intra-orally (Darby and Walsh, 2014).
The plastic manual toothbrush handle may be
bent by placing it above a flame or running the handle under hot water – this will
help to angle the brush bristles against the curve of the arches of the teeth (Darby
and Walsh, 2014).
Built-up
(wider) device handles with different materials to better accommodate those with
a weaker grip strength – such as bicycle grips, Styrofoam molds, and arts-and-crafts
materials. These materials can be used with their toothbrushes and floss
holders and changed when necessary (Darby and Walsh, 2014).
Power
toothbrushes are also recommended for poor dexterity (Darby and Walsh, 2014).
A
universal cuff (Velcro strap) can be attached around the arm or wrist to help
with stabilization (Darby and Walsh, 2014).
Oral
care foam stick dipped in povidone-iodine mouthwash – for about 1 minute to
remove food and plaque remaining on the teeth (Oral care
for the dependent elderly, n.d.).
Spatula-shaped
brush with light scrubbing to clean the tongue (Oral care
for the dependent elderly, n.d.).
Caregivers
may assist in cleaning their dentures daily, as recommended (Oral care
for the dependent elderly, n.d.).
The
dependent seniors positioning may also need accommodating. Those with neuromuscular
disorders may need a stabilization device to avoid them from moving away from their
upright and secure positioning by providing materials such as backrests, headrests,
seatbelts, chest straps, lateral trunk supports and hip guides (Darby and
Walsh, 2014).
For
the individuals who are prone to having seizures, immobilization devices should
be used with caution – should be removed in the event of a seizure (Darby and
Walsh, 2014).
(What are activities of daily living?, n.d.)
For caregivers, some assisting recommendations can be to have the senior sit down, stand beside the senior (not directly in front of them), wrap their arms around the seniors’ head to support their chin/head using their hands (Oral care for dependent seniors, 2019). Continue with gentle oral care. If the senior is unable to open their mouth, the caregiver must do their best to brush anything they can access (Oral care for dependent seniors, 2019). Even if they are only able to brush the anterior part of their teeth and the sides of their teeth facing their cheeks, this will still improve their oral health by an increasing amount (Oral care for dependent seniors, 2019).
Every dependent senior should be assessed for their level of dexterity in order for them to receive the most optimal self oral care as possible, preventing any risks of oral disease (Oral care for dependent seniors, 2019).
JE
References:
Darby and Walsh, 2014. Dental Hygiene: Theory and
Practice (4th Edition) [Texidium version]. Retrieved from http://texidium.com
Dementia impacts the entirety of a senior’s life including memory, behaviour, brain function, language, and everyday functions. (Alzheimer Society Canada, 2018). As it progresses its impact and severity increases. (Alzheimer Society Canada, 2018). As stated previously dementia impacts the daily life of the elderly. When you think of everyday functions you may think of cooking dinner, doing the laundry, using the washroom, driving to the grocery store, or taking medications. One important aspect of daily life impacted by dementia is oral care.
Seniors with dementia may struggle with remembering that they need to brush their teeth or take out their dentures at night. (Alzheimer’s Association, n.d.). It can also influence their ability to perform oral care thoroughly and properly. (Alzheimer’s Association, n.d.). Thus, their oral health can greatly deteriorate as well as their quality of life.
Oral health care is an important daily routine that cannot be skipped. Without proper care your oral health will decline and may manifest as cavities, gingivitis, periodontitis, bad-breath, lost teeth, tooth sensitivity, and oral infections. (ODHA, n.d., p. 1). These undesirable outcomes have a great effect on their quality of life. (Stewart, 2012). For example, it impacts their social abilities whether it is a lack of self-confidence due to unattractive teeth or an inability to speak as well as once before. (Stewart, 2012). The happiness of seniors is jeopardized when oral care is not a priority. The ability to eat is also compromised if there is dental pain or a lack of teeth leading to potential weight loss and malnourishment. (Stewart, 2012). Furthermore, it has been noted oral health is linked to one’s overall health. (ODHA, n.d., p. 1). Poor oral health introduces bacteria into the blood stream. (ODHA, n.d., p. 1). Once in the blood stream these bacteria are brought all around the body. (ODHA, n.d., p. 1). Bacteria from infections in the mouth have the potential ability to increase the likelihood of cardiovascular and respiratory issues. (ODHA, n.d., p. 1). Therefore, it is of great importance that oral health in seniors with dementia is not forgotten because it impacts their overall health and quality of life.
Figure 2: Nursing Staff Helping Resident with Routine Oral Care. (UAB School of Nursing, 2018).
Partners, family members, nursing staff, and dental hygienists have the ability to improve the oral health of seniors thus preventing the repercussions poor oral health brings. It is always important for seniors with dementia to attend regular dental appointments to catch dental issues early and preventing extensive dental procedures in the future. (Alzheimer’s Association, n.d.). You can play a part by booking appointments, driving them to appointments, educating them of why they need regular dental appointments. In the early stages of dementia, it is important to remind the elderly with dementia to brush their teeth using simple instructions. Rather than an ambiguous phrase of “brush your teeth.” (Alzheimer’s Association, n.d.). You may remind them face-to-face or leave notes in their room to remind them to brush their teeth and the steps that the task takes. As it progresses you may choose to guide their oral care to ensure that they are doing their self oral care properly. If it is noticed that they are having difficulty properly performing oral care due to dexterity issues you may want to try a new toothbrush or flossing aid. There are many different modified toothbrushes specifically to increase dexterity and electrical toothbrushes are available as well. Some interdental aids that can be used instead of regular string dental floss are floss picks, floss holders, interdental brushes, water piks, etc. (American Dental Association, 2019). However, as the dementia becomes more severe, care takers and family members be needed to do their oral care for them. (Alzheimer’s Association, n.d.). If this is the case, it is important to remember to communicate with the senior before going ahead and sticking a toothbrush in their mouth. Be sure to ask them and explain what you will do. Then show them what you will use and what you will do. Finally, then you may begin oral care. (ODHA, n.d., p. 2).
Oral care for seniors does not just encompass brushing twice a day with fluoridated toothpaste and flossing. It also includes caring for dentures. It is important that seniors with dentures remove them at night and regularly clean the dentures. (ODHA, n.d., p. 2). Whether the dentures are full or partial it is important to remove them regardless. If they are not removed, they can negatively impact the oral health and overall health of the senior. (ODHA, n.d., p. 2).
Oral care is a large need of seniors living with dementia. It is important to recognize that seniors with dementia may need reminders or help with their daily oral care activities. Whether you’re a family member, a nurse, or a dental hygienist, it is vital that you look out for the oral health in seniors with dementia. You can make a difference in the life of a senior with dementia. You can improve their life quality and prevent further health complications in the future.
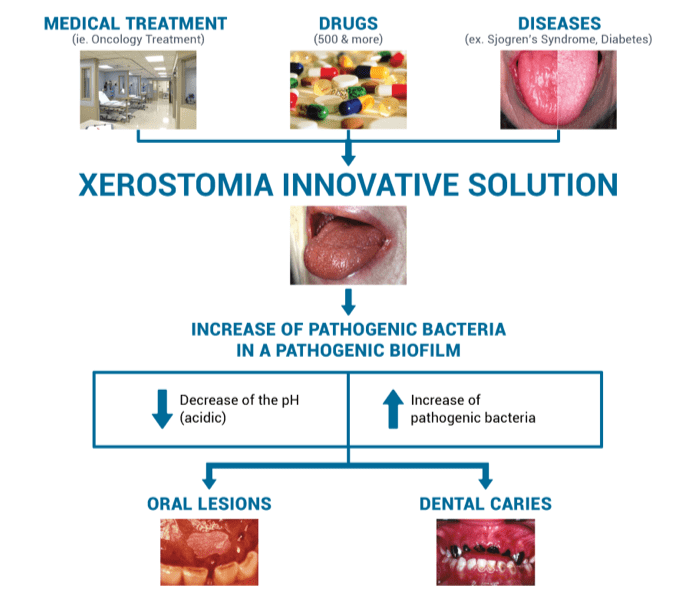
Saliva is a critical component when
it comes to optimal oral health and comfort. Unfortunately, there is 20-50% of
the population that suffers from lack of saliva resulting in a dry mouth (Hemalatha,
2019). The deficiency in saliva is a concern for professionals as it
increases the chances of dental decay and periodontal disease while decreasing
the protective components found in saliva (Huang, 2015).
There are two diagnostic categories for low saliva flow: salivary gland hypofunction and xerostomia (Hemalatha, 2019). Xerostomia is a term that is use when the saliva flow is decreased and the patient expresses symptoms of dry mouth, whereas salivary gland hypofunction is an asymptomatic decrease in saliva. Both are names for a decrease in saliva, the difference being one is symptomatic (xerostomia) and the other is not (SGH) (Hemalatha, 2019).
There are several reasons for one to experience SGH or xerostomia, the following is a list of some potential causes: medications, radiation, age, dentures, chronic disease, etc (Huang, 2015). The most common form of xerostomia or SGH that professionals encounter is a side effect of medication(s). With 80% of all prescription medication having this side effect, and more than 75% of the people aged 65+ taking prescription medication concludes that the xerostomia and/or SGH has a high rate of occurrence in the elderly population (Hemalatha, 2019.
Science, O. (2018)
Radiation of the head and neck is another cause of xerostomia or SGH, this is due to the radiation causing damage to the salivary glands which produce saliva (Hemalatha, 2019). The damage that occurs to the gland will result in fibrosis (comparable to scar tissue) of the gland which prevents it from being able to secrete an adequate amount of saliva (Huang, 2015). Generally, clients will initially notice more viscous saliva in their mouth, followed by a complete loss of any salivary production (Huang, 2015). The amount of damage caused to the salivary glands depends highly on the (Science, 2018)amount of radiation delivered to that site. The more radiation, the more fibrotic the gland will become (W.Little, 2017).
Medications are a large contributing factor to elderly’s experiencing salivary dysfunction; however, it is certainly not the only reason for dry mouth in this population (W.Little, 2017). Recently, there was a study done on a group of seniors in a nursing home in Taiwan to elaborate on this topic (Huang, 2017). There were two divisions of this nursing home – one side is for the ‘nursing’ side (more psychological and more debilitating situations) and the others is the ‘seniors’ side (more self-sufficient but still in need of assistance). The study was done to try and categorize which seniors require more dental care due to their dry mouth condition. The conclusion of the study was that the senior side which required less staffing/help with daily oral care are suffering much more than those on the nursing side which have a practitioner close by most of the time (Huang, 2017). Other contributing factors were the lack of professional dental visits and dentures (not being able to properly clean/care for their dentures and/or tissue below(Huang, 2017).
There are four suggested methods to aid in managing this disease. They are as follows (Hemalatha, 2019).: 1. Palliative measures 2. Saliva Substitutes 3. Drug Switching 4. Drug Therapy
Palliative measures consist of treating any symptoms and being proactive in terms of disease prevention (Hemalatha, 2019). Methods used for this treatment is focused on homecare regimens: proper brushing/flossing, removing any plaque/food debris that saliva would generally clear, reducing intake of highly acidic food, reduce frequency of acid attacks in the mouth (not snacking all day), use of at home fluoride rinses and pastes (Hemalatha, 2019)..
Second management option is the use of salivary substitutes and/or lubricants (Hemalatha, 2019).. There are saliva substitutes that are sold over the counter that consist of all the same components regular saliva consists of. This is a highly recommended method as the salivary substitute consists of the same chemical/physical components of saliva (Hemalatha, 2019). Therefore, it has the ability to demineralize teeth after an acid attack, break down any harmful bacteria/build up in the mouth, and protect the structures inside the oral cavity to aid in disease prevention(Hemalatha, 2019).
Now let’s review the use of drugs to help manage SGH/xerostomia. Ideally, medical professionals would recommended drugs without this side effect or find an alternative with less chance of this side effect (Hemalatha, 2019). However, that is not realistic and the control of systemic disease takes priority. It is always an option to consult a medical professional if one is experiencing complications with dry mouth to explore alternative options (W. Little, 2017).
Lastly, the use of drugs to help stimulate salivary flow: Pilocarpine Hydrochloride (Hemalatha, 2019). This is a medication that stimulates salivary flow by mimicking the body’s natural pathway of creating saliva. The drug works on the brain that sends signals to the salivary glands to release more saliva (Hemalatha, 2019). There are different types and dosage depending on the client. This is a medication that is generally needed to be taken consecutively for optimal results (Hemalatha, 2019).. Like all medication, there are side effects to pilocarpine hydrochloride and it is advised that one consults their medical professional to ensure this medication is appropriate for them (Hemalatha, 2019).
How to manage SGH or Xerostomia (Huang, 2017) -Regular professional dental visits -Appropriate preventative care (fluorides, counselling, debridement, etc) -Use of sugar free gum and/or salivary substitutes -Keep hydrated -Use fluoride tooth paste/mouth wash -Ensure proper homecare is being done (with assistance if needed)
To conclude, when one is diagnosed with SGH and xerostomia it will affect many aspects of their life and it truly does result in a decrease in quality of life. Saliva aids in speech, eating and comfort which are part of our everyday tasks (Huang, 2017). Although this disease may be inevitable for some, there are certainly ways to manage it so that one can enjoy their life while maintaining health and comfort.
In summary, the following are list taken from the Oral Science website to aid is understanding and managing salivary gland hypofunction or xerostomia (Science, 2018):
CLINICAL SIGNS OF XEROSTOMIA (SCIENCE, 2018)
-Burning sensation -Food sticks to mucosa -Oral health problems / Tissue alterations -Angular chellitis (corner of lip sores/inflammation -Candidiasis (fungal infections) -Caries (Cavities) -Halitosis (Bad breath) -Loss of filiform papillae on tongue (Shining appearance of tongue) -Mucositis (Inflamed, sore tissues in the mouth) -Oral lesions -Pain -Periodontal disease (Gum disease) -Redness of the tongue -Taste alteration -Tooth sensitivity
FUNCTION OF SALIVA (Science, 2018):
-Acting as a buffer to neutralize acidic challenge -Aiding in immune response with the presence of proteins, cytokines, hormones and mucins -Aiding in proper speech and articulation -Delivering calcium, phosphate and fluoride -Performing as a lubricating agent -Playing an active role in elimination of food and bacteria -Protecting exposed root surfaces
CLINICAL SIGNS OF XEROSTOMIA (SCIENCE, 2018) -Burning sensation -Food sticks to mucosa -Oral health problems / Tissue alterations -Angular chellitis (corner of lip sores/inflammation -Candidiasis (fungal infections) -Caries (Cavities) -Halitosis (Bad breath) -Loss of filiform papillae on tongue (Shining appearance of tongue) -Mucositis (Inflamed, sore tissues in the mouth) -Oral lesions -Pain -Periodontal disease (Gum disease) -Redness of the tongue -Taste alteration -Tooth sensitivity
ADVICE WITH XEROSTOMIC PATIENTS (SCIENCE, 2018): -Changing or modification of the medications’ dosage -Drink milk while eating -Frequent dental exams -Frequent hydration (sip water regularly) unless there’s cause not to: Severe restrictions from cardiac and renal problems -Humidification of the bedroom -If no risk of choking: sucking on ice cubes or frozen juice bars -Mash, humid food with light touch of citrus -Rigorous dental hygiene
TO AVOID WITH XEROSTOMIC PATIENTS (SCIENCE, 2018): -Alcohol -Coffee -Highly acidic food -Sweet food -Tobacco
James W. Little, Donald Falace, Craig Miller, Nelson L. Rhodus. (2017). Dental Management of the Medically Compromised Patient (9th Edition) [Texidium version]. Retrieved from http://texidium.com
Healthy seniors tend to keep their teeth throughout their lifetime. However, the presence of medical condition can alter and impact a senior’s oral and systemic health. 30% of those who were between 65 – 74 years in 1986, were edentulous (lack of teeth) and it was estimated that in 2024, only 10% of this group will be edentulous (Garcia, Harris & Nathe, 2013, p. 426). The declination in tooth loss results in an increased risk of caries (Garcia et al., 2013, p.426). Thus, this tells us that as our senior population are retaining more teeth, there needs to be an adequate sequence of oral hygiene home care known to the senior population and those who care for our dependent seniors.
Prevention and maintenance specifically for dependent seniors who live in long- term care (LTC), is extremely crucial to increase their quality of life. Many LTC residence can take care of their own oral hygiene; however, for those seniors who are primarily dependent on their caregiver, their needs are usually taken care of by nurses and dental professionals who are either on site or who provide mobile dental care. Seniors in LTC have been known to have high risk for edentulism, coronal and root caries, poor oral hygiene, periodontal disease and soft tissue lesions (Garcia et al., 2013, p. 427).
Regular dental exams, effective tooth brushing and flossing are important steps in maintaining optimal oral health.
Toothbrush Technique
A soft bristle toothbrush is always recommended in order to prevent any gum trauma; choosing a correct size would also allow proper and easy access to back area of the mouth.
Step 1: Place the bristles of the toothbrush at a 45-degree angle towards the gum. Using gentle circle vibration motions followed by a sweeping motion towards the biting surface (Canadian Dental Association, n.d.).
Figure 1: Modified bass method (Garcia et al., 2013, p. 139)
Avoid scrubbing and putting too much pressure: this can cause the gums to recede.
Step 2: Ensure that all surfaces (biting surfaces as well) are brushed along with the cheek and tongue. Brushing the tongue removes the bacteria that has accumulated on the surface; this accumulation contributes to breath malodor. The recommendation for brushing should take place for 2 minutes (Canadian Dental Association, n.d.).
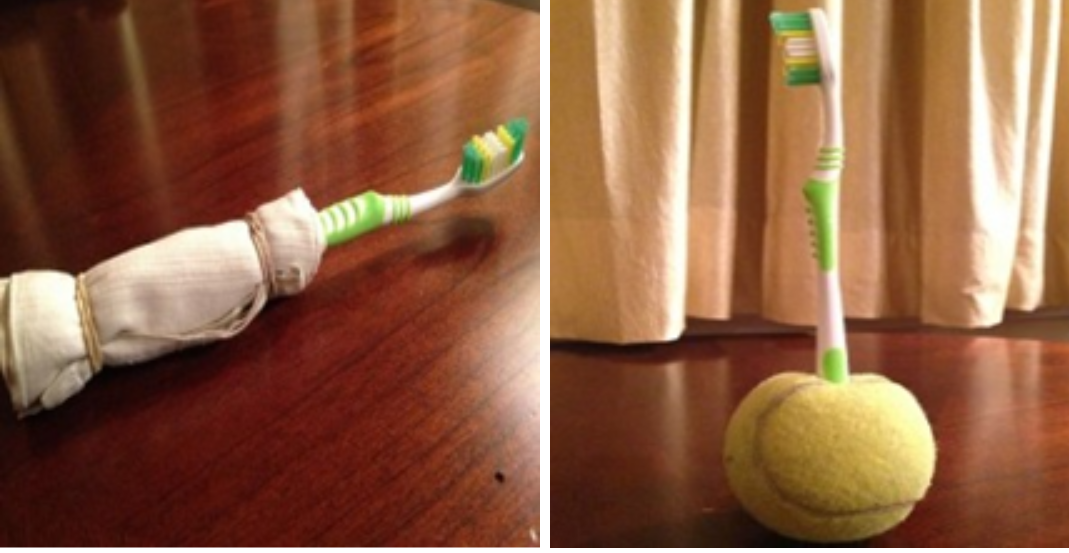
Modified toothbrush handles
Some seniors are able to provide their own oral hygiene care; however, some seniors may face difficulties due to dexterity problems that may be due to arthritis or other health conditions. Here are some tips on how to ensure that those with dexterity issues can still achieve a thorough and effective tooth brushing.
Having a larger surface area to grip is much easier than gripping a small toothbrush handle. Enlarging the area by adding a sponge, cloth or tennis ball to the handle makes it easier for it to hold (Exceptional Smiles, n.d.).
Figure 2: Adaptations for toothbrush (Exceptional Smiles, n.d.)
Flossing technique
There are many flossing aids out there such as proxabrush, waterpik, floss picks, etc. Each senior may require a different aid that is comfortable for them according to their needs.
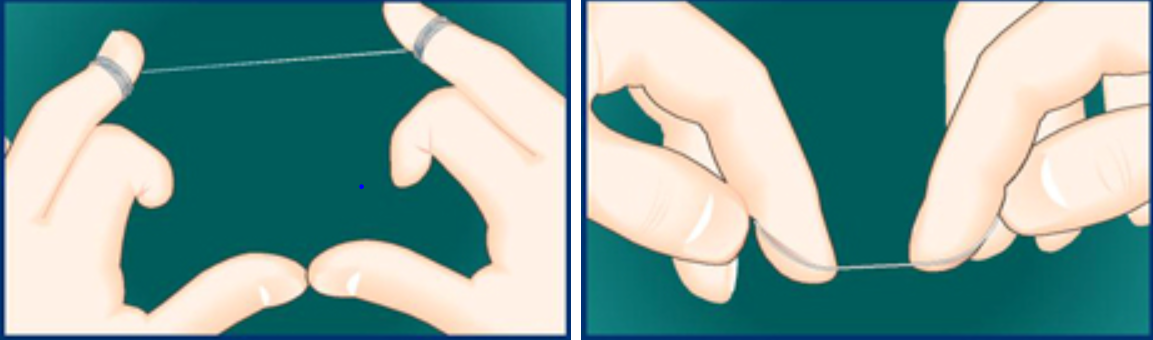
Brushing alone is not enough to ensure adequate plaque removal. Floss reaches those areas that the bristles of the toothbrush are not able to reach such as in between your teeth and 1-3 mm underneath the gum (Canadian Dental Association, n.d.) .
Step 1: Retrieve floss approximately a foot-long. Wrap it around both your middle fingers leaving an inch in space. The floss will be guided by the index fingers and/or thumbs (Canadian Dental Association, n.d.).
Step 2: Gently see-saw the floss in between the teeth and once it is in wrap it around one side of the tooth into a “C- shape”. Gentle go up and down for two to three times, making sure to go underneath the gum line (Canadian Dental Association, n.d.). Before snapping the floss out, ensure that the adjacent surface is also cleaned.
Seniors who suffer from xerostomia (dry mouth) whether it is due to medical conditions, medications or other causes, should include a mouth rinse in their daily oral hygiene routine. Mouthrinses that are commonly used for xerostomia include: Oasis mouthwash by Sensodyne, Biotène mouthwash and Orazyme Dry Mouth mouthwash (Garcia et al., 2013, p. 156).
By doing these steps, seniors will have an adequate oral hygiene routine care which is important in maintaining their quality of life. Those who care for dependent seniors are required to have adequate knowledge not only on their systemic health, but oral health as well. Lastly, regular dental professional care is necessary in order to maintain optimal oral health.
As
we know, many dependent seniors wear dentures. What are dentures? A denture is
an artificial material that mimics teeth and gums as a replacement (What are dentures?, 2019).
Dentures
are considered to restore oral functions (including missing teeth and bone
resorption) and to restore the facial features around the mouth (Darby, &
Walsh, 2014, p.1006).
There
are different types of dentures made in a laboratory to meet the needs of individual
seniors as listed below:
Partial denture -> replaces only some and not all missing teeth and gums. Can be removed and placed back into the mouth by the client. The partial denture rests on metal framework (retainer clasps) and is supported by natural teeth when placed inside the mouth (Darby, & Walsh, 2014, p. 1007).
Full/complete denture -> replaces all teeth and gums of either the upper or lower arch. Can be removed and placed back into the mouth by the client (Darby, & Walsh, 2014, p. 1008).
Caring
for the denture includes removing the denture to clean after eating and before
bed. Brushing the denture with a cleaning solution and a denture brush daily
will avoid microorganisms from harvesting on to the denture and remaining
inside the oral cavity. Soaking the dentures before bed time in water with a
mild overnight cleanser will remove the bacteria (which also removes the odour)
and the moisture will stabilize the shape of the denture. (Proper Denture Care and Maintenance, 2019)
(Dental Use
and Care Instructions, n.d.)
(Dental Use
and Care Instructions, n.d.)
The
advantages for dependent seniors with dentures are the following:
Seniors will
have a full functioning set of teeth to assist with smiling, speaking and
chewing solid foods (What are the benefits of dentures?, n.d.)
Have them look and
feel much better about their overall appearance (without the ‘sunken cheek’ appearance)
(What are the benefits of dentures?, n.d.)
Can last for a long
time only if taken care properly – around 5-10 years (Dentures: Their Advantages and Disadvantages, 2019)
Although
dentures can be a huge advantage to many, there are many disadvantages to
consider, as listed below:
Dentures tend to
move around in the mouth, which can become irritable when chewing or speaking
(will need some getting used too) (What are the benefits of dentures?, n.d.)
Denture care needs
to be addressed as important as caring for natural teeth to avoid any bacteria
build up (What are the benefits of dentures?, n.d.)
Masticatory
stress (pressure in the mouth from the denture) can result in continuing
alterations to the gums and oral cavity (Darby, & Walsh, 2014, p. 1010).
There are risks
of having inflammation and lesions in the mouth, if not removed and cleaned
properly (Darby, & Walsh, 2014, p. 1010).
Bacteria left on
denture built up can cause periodontal disease – first signs being tartar at
the base of the teeth, which then lead to tissues of the teeth and gums being destroyed
(Oral Care for the Elderly, n.d.)
Dependent
seniors may not be caring for their dentures as often or adequately as they
should be and that can be due to many reasons; such as the family member or
caregiver is unable to care for the senior adequately and/or regular dental
visits for them decrease or cease over time (Our health system neglects the oral health of
dependent seniors with tragic consequences, 2017).
When
caregivers and/or family members are providing the care for others, it requires
a skill with the responsibility and resources to do the care regularly and properly
(Our health system neglects the oral health of
dependent seniors with tragic consequences, 2017). While the registered
nurses of Ontario have a guideline called “Oral Health Nursing Best Practice Guidelines”
that they follow to ensure proper daily oral care is being performed for the
dependent seniors, it is important that the seniors and family members
understand the importance and are as well educated on the concerns (Our health system neglects the oral health of
dependent seniors with tragic consequences, 2017).
The
following listed below must be taken into consideration for the caregiver and
family member in order to avoid any problems in oral cavity of the dependent senior:
Dental visits
regularly (Caring for Dentures tips for Seniors and Caregivers,
n.d.)
Encouraging the seniors
to remove and clean on their own with support if needed (Caring for
Dentures tips for Seniors and Caregivers, n.d.)
Avoid cross-contamination
by wearing gloves (Caring for Dentures tips for Seniors and Caregivers,
n.d.)
First remove the
lower by holding the front teeth between the thumb and index finger and then
lifting it out. Next remove the upper denture by lifting the lip and using
fingers to tip the front teeth (rocking the denture back and forth may help
remove the seal) (Caring for Dentures tips for Seniors and Caregivers,
n.d.)
Carefully remove
partial dentures by using fingers and gently pulling the metal clasps away from
the teeth (either downward or upward motion) (Caring for Dentures tips for Seniors and Caregivers,
n.d.)
Remember to inspect
the mouth for any sore spots that do not heal in a few days, white or red
patches, or any changes of colour in the mouth. These concerns may need to be
addressed to a dentist (Tips for Caregivers, 2019).
Assist with proper
denture cleaning performed as listed before and clean any natural teeth if any
are remaining (Caring for Dentures tips for Seniors and Caregivers,
n.d.)
Clean by
massaging the inside of seniors’ mouth using a damp cloth or a soft toothbrush (Tips for Caregivers, 2019)
Encourage the senior
to reinsert the denture or assist if help is needed (Caring for
Dentures tips for Seniors and Caregivers, n.d.)
By
doing these important necessary steps, this will reduce the risks of any concerns,
the seniors will feel more confident and will keep smiling!
Figure 1: Senior Citizen and Care Provider (Sunnybrook Foundation, n.d.)
Today we’re going to be discussing the lack of funding for oral care in dependant seniors. Seniors in Canada are a population that are increasing at a rapid rate making up for a large portion of our total population, “In 2014, over 6 million Canadians were aged 65 or older, representing 15.6 percent of Canada’s population. By 2030—in less than two decades—seniors will number over 9.5 million and make up 23 percent of Canadians” (Social Development Canada, 2019, p.1). Seniors make up such a significant part of our population and given the many risk factors and obstacles present regarding oral health in this population, regular oral health care is vital. Some of the obstacles that this population faces include:
· Anxiety and fear of new situations or procedures may affect willingness to seek dental care (Marvin, 2001, p.1).
· Compromised immune systems (Darby & Walsh, 2014, p.263).
· Decreased cognitive ability, medications and limited ability to tolerate procedures may reduce the desire for care (Marvin, 2001, p.1).
· Decreased salivary flow (often a side effect of many common medications) (Darby & Walsh, 2014, p.263).
· Dietary habits (Darby & Walsh, 2014, p.263).
· Existing esthetic factors, including missing teeth, may contribute to a reluctance to go out in public (Marvin, 2001, p.1).
· Socioeconomic status (Darby & Walsh, 2014, p.263).
· Lack of funding (Darby & Walsh, 2014, p.263).
· Lack of water fluoridation the early years of life resulting in higher predisposition to cavities (CDC, 2016).
· Limited dexterity resulting in insufficient oral hygiene technique and plaque removal (Darby & Walsh, 2014, p.263).
· Poor overall health can restrict access to care (Marvin, 2001, p.1).
· Seniors may be unable or unwilling to be transported off-site to a treatment centre (Marvin, 2001, p.1).
For several of the reasons listed above, the need for regular dental visits in this population is crucial. “Unfortunately, Canada also has one of the lowest rates of publicly funded dental care in the world, and since almost all dental care is funded privately through employer-based insurance (or out of pocket), non-coverage becomes an issue as people age and retire” (Fowler, 2019, p.1). For many in this population oral care is no longer a service they can afford. Often retired seniors are no longer receiving nearly as much of an income, if they are even lucky enough to be receiving a pension. Along with a reduced income, seniors that did have dental insurance during their working years are no longer covered. With the reduced income they now having to survive off of sadly oral health care often doesn’t make the cut despite the need for it. Arlene Henderson, a low-income senior resident, reports losing several teeth and now requiring major dental “I had to have some dental work done, but I can’t get it done because it’s too expensive,” (CBC, 2018, p.1). Unfortunately, Arlene’s situation is far more common than we would like to think, her $1,000 monthly income makes it difficult to afford basic human needs let alone additional dental care that will only get worse the longer it goes untreated (CBC, 2018, p.1).
When looking at dental care for the population of Ontario as a whole, there are several government funded programs allocated to other populations such as Healthy Smiles for children or ODSP Adult (Ontario Disability Support Program). “The Healthy Smiles Program is an Ontario government-funded basic dental program providing preventive and early treatment services for children and youth in low income families, who are 17 years of age or under. If eligible, your children will get regular dental services at no cost to you” (Health n’ Smiles, n.d., p.1).
All of the above leads us to the question, when will dependant seniors receive the funding they need? Thankfully due to the support and advocacy on behalf of this population it looks like change is on the horizon. On Tuesday, April 23, 2019
Ontario announced “it will be investing $90 million in dental care for seniors 65 and over. If you’re a senior earning less than $19,300 per year or a couple earning a combined income of $32,300 or less without dental benefits, you will qualify for the Ontario Seniors Dental Care Program” (Settlement Ontario, 2019, p.1). What exactly this program will cover is still yet to be confirmed, however we’re beyond excited to see a step in the right direction.
Figure 1: Oral Cancer Screenings at Medical Office. (Kalil&Kress Family and Cosmetic Dentistry, n.d.).
Did you know that oral cancer ranks as “the sixth most common cancer.”? (Atherley, Taylor & Aquilina-Arnold, 2010, p.7). Oral cancer is found in the oral cavity, otherwise known as the mouth. Though oral cancer may begin in the oral cavity it may develop within nearby or farther regions of the body. This spread of oral cancer to farther bodily regions is called metastasis. (Canadian Cancer Society, n.d.). Oral cancer is greatly impacting the elderly in our society. Oral cancer instances greatly increase with age. (Laronde, Hislop, Elwood & Rosin, n.d., p.2). In a journal article published by Canadian Journal of Dental Hygiene, it states those at the greatest risk for oral cancer are over the age of sixty. (Laronde et al., n.d., p.1). Therefore, your aging loved ones are placed at higher risk.
There is no single causative factor that causes oral cancer to begin. However, there are multiple risk factors that may impact cancerous formations. As many may already know, tobacco greatly increases the likelihood of cancer formation whether in oral cavity or other areas of the body. (Laronde et al., n.d., p. 2). Furthermore, the use of tobacco and excessive alcohol are strong risk factors that together increase the chances of developing oral cancer. (Laronde et al., n.d., p. 2). Other risk factors include a lack of fruits and vegetables incorporated in to a regular diet, Human Papilloma Virus, and excessive exposure to UV rays. (ODHA, n.d., p. 1).
Early detection and diagnosis are of great importance. Greater survival rates are seen within cases where oral cancer was spotted early. (Laronde et al., n.d., p. 1). This is why family members, seniors, nursing staff, and dental hygienists must be aware of the increased risk for oral cancer in the elderly. Early detection can save your loved one’s life. Regular oral cancer screenings for seniors by themselves, family members, dental hygienists, PSWs, etc., can help in the early detection and diagnosis.
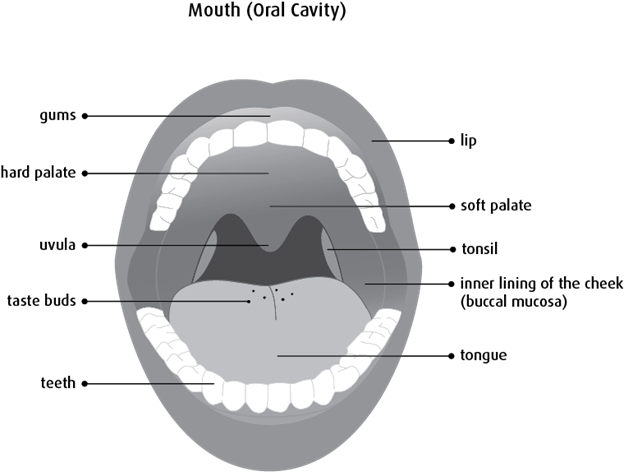
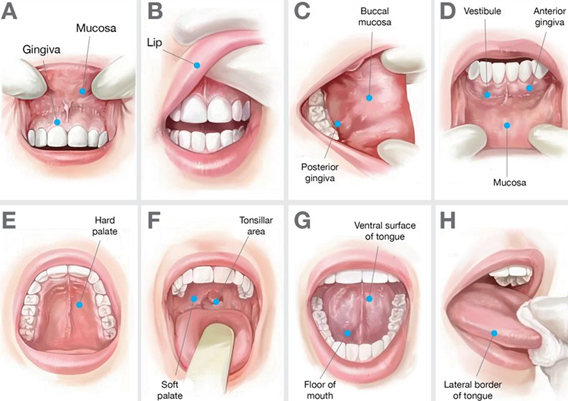
Figure 2: Anatomy of the Oral Cavity. (Canadian Cancer Society, n.d.).
“What is oral cancer screening?” you might ask. Oral cancer screenings are a sequence of steps used to observe any changes inside and outside of the mouth. Oral cancer is not normal, therefore, any unusual lesions or changes in the mouth may indicate precancerous or cancerous formations. Changes such as:
– non-healing sores on the lips or in the mouth (National Cancer Institute, 2019).
– white patches (National Cancer Institute, 2019).
– red patches (National Cancer Institute, 2019).
– colour changes within the mouth (National Cancer Institute, 2019).
– voice changes (National Cancer Institute, 2019).
– difficulty moving the tongue (National Cancer Institute, 2019).
– difficulty speaking or swallowing (National Cancer Institute, 2019).
– lumps within the lips or mouth (National Cancer Institute, 2019).
– numbness in the lips or mouth (National Cancer Institute, 2019).
– loose teeth (National Cancer Institute, 2019).
– ill-fitting dentures (National Cancer Institute, 2019).
– lumps within the throat or sore throat (National Cancer Institute, 2019).
– constant earache (ODHA, n.d., p. 1).
– Any unevenness in the face called asymmetry (ODHA, n.d., p. 1).
– lymph nodes that have become solid and immoveable (ODHA, n.d., p. 1).
If these changes are noted to last for two weeks or longer, it is recommended that a consultation be made with their dentist or physician. (ODHA, n.d., p. 1). Bringing this information to the attention to the dentist or medical physician is important. Whether or not this change or growth is cancerous it is better to have a professional opinion than not report anything at all.
As elderly individuals, family members, friends, nursing staff, dental hygienists who are knowledgeable on the increased risk of oral cancer in the elderly you have an important role of observation and communication. Though oral cancer screening sounds daunting, the steps are simple to follow.
1. Look at and around and touch the face. Do you notice any changes in colouring, touch, or symmetry? (ODHA, n.d., p. 2). Look around the back of the neck, ears, and scalp as well. A tip when observing the face is to remove glasses because they may cover up potentially cancerous changes. (ODHA, n.d., p. 2).
2. Listen for changes or complaints that the senior might have. (ODHA, n.d., p. 2). Is their throat hoarse? Are they complaining about a lump in their throat or that their dentures aren’t fitting properly? (ODHA, n.d., p. 2).
3. Go intra-orally (into the mouth). If you are performing this on a senior it is recommended that you wear gloves and using a flashlight when assessing their mouths. If the senior has a denture or other oral appliance kindly ask them to remove it prior to beginning your intra-oral assessment. (ODHA, n.d., p. 2). Take a look and feel around in the mouth. Is there anything unusual or different that you see such as a colour change, a swelling, a sore spot? (ODHA, n.d., p. 2). A tip when observing the mouth is to follow a pattern that you can remember so that no area goes unnoticed.
Figure 3: Oral Cancer Screening Steps.(HealthCare Global, 2018).
Areas in the mouth that are important to assess are:
– The lips – the outside and inside (ODHA, n.d., p. 2).
– The gums (ODHA, n.d., p. 2).
– The entire tongue – front, back, bottom, sides (ODHA, n.d., p. 2).
– The floor of the mouth (the area between the bottom teeth and the tongue). (ODHA, n.d., p. 2).
– The cheeks (ODHA, n.d., p. 2).
– The roof of the mouth also called the palate (ODHA, n.d., p. 2).
– The back of the throat (ODHA, n.d., p. 2).
You can save a life; you have to power to improve a senior’s life. Let’s protect our seniors through early detection. If you had oral cancer, wouldn’t you want it to be caught early? Our seniors need you and need to be educated on the risks of oral cancer.
Laronde, D. M., Hislop, T. G., Elwood, J. M., Rosin, M. P. (n.d.). Oral cancer: just the facts. Canadian Journal of Dental Hygiene. 74 (3), 269-272.Retrieved May 10, 2019 from https://cda-adc.ca/jcda/vol-74/issue-3/269.pdf
Today I’ll be talking about a large concern for oral health in the population of dependant seniors, root caries (caries is another word for cavities). First and foremost, what are root caries? According to Darby & Walsh “Root caries is dental caries involving the tooth root, cementum, or cervical area of the tooth. Root caries is found most frequently in the elderly population, in whom root exposure is common because of gingival recession” (Darby & Walsh, 2014, p.263)
To better understand the significance of root caries/cavities you need the basic knowledge of what a cavity is and how they form. A cavity forms on a susceptible tooth when there are cavity causing bacteria called cariogenic bacteria present. The bacteria consumes carbohydrates from your diet and create acid. These acids as a result wear away and weaken the tooth creating a cavity (Darby & Walsh, 2014, p.261). Caries are a bacterial infection where the bacteria slowly wears away at the tooth structure and starting from the outermost layer called enamel into the second layer called dentin and eventually into pulp chamber if not treated in time (Darby & Walsh, 2014, p.261). Once the cavity progresses into the dentin some sensitivity to hot, cold or sweets may be felt (Darby & Walsh, 2014, p.267). If the cavity progresses to the pulp chamber pain may be experienced because this is where the nerves of the tooth are found (Darby & Walsh, 2014, p.267). Unfortunately, this disease is only reversible at the very first stage of progression and without regular dental visits for seniors the opportunity to stop the disease from progressing often gets missed.
The signs and symptoms of a cavity greatly depend on the location and extent of cavity progression. In the beginning stages of cavity formation symptoms may go unnoticed however as it further progresses some sign and symptoms may include:
Toothache, spontaneous pain or pain that occurs without any apparent cause (Mayo Clinic, 2017).
Tooth sensitivity (to hot or cold) (Mayo Clinic, 2017).
Mild to sharp pain when eating or drinking something sweet (Mayo Clinic, 2017).
Visible holes or pits in your teeth (Mayo Clinic, 2017).
Brown, black or white staining on any surface of a tooth (Mayo Clinic, 2017).
Pain when you bite down (Mayo Clinic, 2017).
You might be wondering to yourself why are root caries such a predominate issue in the dependant senior population? You may be surprised by many of the factors that make this population so at risk. Dependant seniors are particularly a high risk population for root caries due to several reasons including more frequent root exposure as a result of gingival recession, decreased salivary flow which is often a side effect of many common medications, compromised immune systems, dietary habits, knowledge deficit, socioeconomic status, lack of regular dental visits/funding, and limited dexterity resulting in inefficient oral hygiene technique and plaque removal (Darby & Walsh, 2014, p.263). One of the largest factors to take into consideration is that the current population of dependant seniors did not fully experience the benefits of water fluoridation “one of the 10 great public health achievements of the 20th century” (CDC, 2016) as it only began in 1945 and has been attributed to a 25% decrease in cavities in both children and adults. (CDC, 2016).
Unfortunately tooth structure cannot restore itself so it is important for us to try to preserve the tooth structure to the best of our ability and focus on a preventative approach. Root caries can be prevented through regular oral hygiene home care (proper brushing and flossing), regular dental visits, fluoridated water/products/treatments, avoiding frequent snacking (minimizing acid attacks), consuming a non-cariogenic diet and using antibacterial treatments such as mouth rinses (Darby & Walsh, 2014). It is important for us to preserve tooth structure for several reasons including aesthetic purposes which are often linked with self-esteem, freedom from pain that may arise with the progression of the cavity, saving time as practicing proper oral hygiene care daily can prevent the need for treatment of cavities and cost – preventative care such as regular oral hygiene practice can alleviate the need for restorative treatment.
Once the cavity has progressed past the initial stage, known as an incipient lesion, it becomes irreversible. The treatment for caries is having the dentist remove the decayed portion of the tooth and restore the void area with restorative dental material, most commonly known as a filling. The filling may be made of the following materials:
Another factor to take into consideration is the financial burden that comes along with restorative dental treatments. Regrettably, often dependant seniors do not have the means, funding or access to the dental care they may require and quite frankly it often is not a priority despite the many implications that arise as a result of cavities.
A few steps that can be taken by family members and nursing staff are: reminding seniors to practice proper oral hygiene care, providing seniors with the proper oral hygiene aids (taking manual dexterity and physical limitations into consideration), helping them perform oral hygiene, providing them with transportation to dental appointments and getting educated to know what to signs and symptoms to look for and when booking an appointment to the dentist is necessary.