
Saliva is a critical component when it comes to optimal oral health and comfort. Unfortunately, there is 20-50% of the population that suffers from lack of saliva resulting in a dry mouth (Hemalatha, 2019). The deficiency in saliva is a concern for professionals as it increases the chances of dental decay and periodontal disease while decreasing the protective components found in saliva (Huang, 2015).
There are two diagnostic categories for low saliva flow: salivary gland hypofunction and xerostomia (Hemalatha, 2019). Xerostomia is a term that is use when the saliva flow is decreased and the patient expresses symptoms of dry mouth, whereas salivary gland hypofunction is an asymptomatic decrease in saliva. Both are names for a decrease in saliva, the difference being one is symptomatic (xerostomia) and the other is not (SGH) (Hemalatha, 2019).
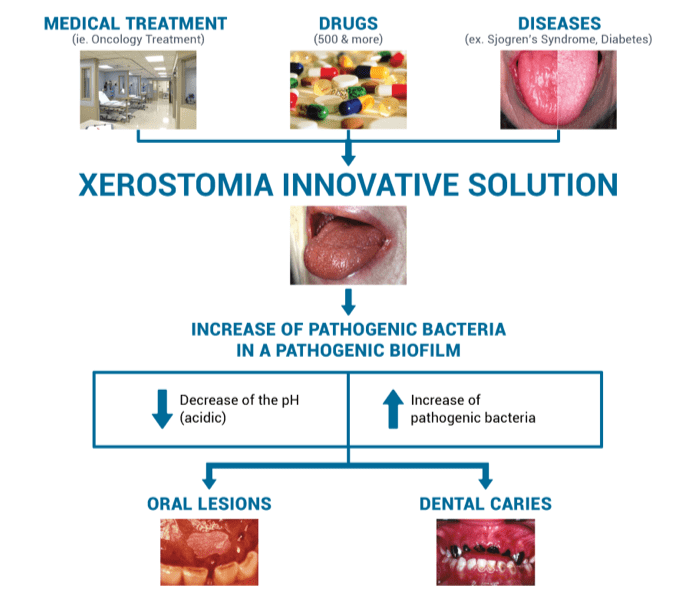
There are several reasons for one to experience SGH or xerostomia, the following is a list of some potential causes: medications, radiation, age, dentures, chronic disease, etc (Huang, 2015). The most common form of xerostomia or SGH that professionals encounter is a side effect of medication(s). With 80% of all prescription medication having this side effect, and more than 75% of the people aged 65+ taking prescription medication concludes that the xerostomia and/or SGH has a high rate of occurrence in the elderly population (Hemalatha, 2019.
Science, O. (2018)
Radiation of the head and neck is another cause of xerostomia or SGH, this is due to the radiation causing damage to the salivary glands which produce saliva (Hemalatha, 2019). The damage that occurs to the gland will result in fibrosis (comparable to scar tissue) of the gland which prevents it from being able to secrete an adequate amount of saliva (Huang, 2015). Generally, clients will initially notice more viscous saliva in their mouth, followed by a complete loss of any salivary production (Huang, 2015). The amount of damage caused to the salivary glands depends highly on the (Science, 2018)amount of radiation delivered to that site. The more radiation, the more fibrotic the gland will become (W.Little, 2017).
Medications are a large contributing factor to elderly’s experiencing salivary dysfunction; however, it is certainly not the only reason for dry mouth in this population (W.Little, 2017). Recently, there was a study done on a group of seniors in a nursing home in Taiwan to elaborate on this topic (Huang, 2017). There were two divisions of this nursing home – one side is for the ‘nursing’ side (more psychological and more debilitating situations) and the others is the ‘seniors’ side (more self-sufficient but still in need of assistance). The study was done to try and categorize which seniors require more dental care due to their dry mouth condition. The conclusion of the study was that the senior side which required less staffing/help with daily oral care are suffering much more than those on the nursing side which have a practitioner close by most of the time (Huang, 2017). Other contributing factors were the lack of professional dental visits and dentures (not being able to properly clean/care for their dentures and/or tissue below(Huang, 2017).
There are four suggested methods to aid in managing this disease. They are as follows (Hemalatha, 2019).:
1. Palliative measures
2. Saliva Substitutes
3. Drug Switching
4. Drug Therapy
Palliative measures consist of treating any symptoms and being proactive in terms of disease prevention (Hemalatha, 2019). Methods used for this treatment is focused on homecare regimens: proper brushing/flossing, removing any plaque/food debris that saliva would generally clear, reducing intake of highly acidic food, reduce frequency of acid attacks in the mouth (not snacking all day), use of at home fluoride rinses and pastes (Hemalatha, 2019)..
Second management option is the use of salivary substitutes and/or lubricants (Hemalatha, 2019).. There are saliva substitutes that are sold over the counter that consist of all the same components regular saliva consists of. This is a highly recommended method as the salivary substitute consists of the same chemical/physical components of saliva (Hemalatha, 2019). Therefore, it has the ability to demineralize teeth after an acid attack, break down any harmful bacteria/build up in the mouth, and protect the structures inside the oral cavity to aid in disease prevention(Hemalatha, 2019).
Now let’s review the use of drugs to help manage SGH/xerostomia. Ideally, medical professionals would recommended drugs without this side effect or find an alternative with less chance of this side effect (Hemalatha, 2019). However, that is not realistic and the control of systemic disease takes priority. It is always an option to consult a medical professional if one is experiencing complications with dry mouth to explore alternative options (W. Little, 2017).
Lastly, the use of drugs to help stimulate salivary flow: Pilocarpine Hydrochloride (Hemalatha, 2019). This is a medication that stimulates salivary flow by mimicking the body’s natural pathway of creating saliva. The drug works on the brain that sends signals to the salivary glands to release more saliva (Hemalatha, 2019). There are different types and dosage depending on the client. This is a medication that is generally needed to be taken consecutively for optimal results (Hemalatha, 2019).. Like all medication, there are side effects to pilocarpine hydrochloride and it is advised that one consults their medical professional to ensure this medication is appropriate for them (Hemalatha, 2019).
How to manage SGH or Xerostomia (Huang, 2017)
-Regular professional dental visits
-Appropriate preventative care (fluorides, counselling, debridement, etc)
-Use of sugar free gum and/or salivary substitutes
-Keep hydrated
-Use fluoride tooth paste/mouth wash
-Ensure proper homecare is being done (with assistance if needed)
To conclude, when one is diagnosed with SGH and xerostomia it will affect many aspects of their life and it truly does result in a decrease in quality of life. Saliva aids in speech, eating and comfort which are part of our everyday tasks (Huang, 2017). Although this disease may be inevitable for some, there are certainly ways to manage it so that one can enjoy their life while maintaining health and comfort.
In summary, the following are list taken from the Oral Science website to aid is understanding and managing salivary gland hypofunction or xerostomia (Science, 2018):
CLINICAL SIGNS OF XEROSTOMIA (SCIENCE, 2018)
-Burning sensation
-Food sticks to mucosa
-Oral health problems / Tissue alterations
-Angular chellitis (corner of lip sores/inflammation
-Candidiasis (fungal infections)
-Caries (Cavities)
-Halitosis (Bad breath)
-Loss of filiform papillae on tongue (Shining appearance of tongue)
-Mucositis (Inflamed, sore tissues in the mouth)
-Oral lesions
-Pain
-Periodontal disease (Gum disease)
-Redness of the tongue
-Taste alteration
-Tooth sensitivity
FUNCTION OF SALIVA (Science, 2018):
-Acting as a buffer to neutralize acidic challenge
-Aiding in immune response with the presence of proteins, cytokines, hormones and mucins
-Aiding in proper speech and articulation
-Delivering calcium, phosphate and fluoride
-Performing as a lubricating agent
-Playing an active role in elimination of food and bacteria
-Protecting exposed root surfaces
CLINICAL SIGNS OF XEROSTOMIA (SCIENCE, 2018)
-Burning sensation
-Food sticks to mucosa
-Oral health problems / Tissue alterations
-Angular chellitis (corner of lip sores/inflammation
-Candidiasis (fungal infections)
-Caries (Cavities)
-Halitosis (Bad breath)
-Loss of filiform papillae on tongue (Shining appearance of tongue)
-Mucositis (Inflamed, sore tissues in the mouth)
-Oral lesions
-Pain
-Periodontal disease (Gum disease)
-Redness of the tongue
-Taste alteration
-Tooth sensitivity
ADVICE WITH XEROSTOMIC PATIENTS (SCIENCE, 2018):
-Changing or modification of the medications’ dosage
-Drink milk while eating
-Frequent dental exams
-Frequent hydration (sip water regularly) unless there’s cause not to: Severe restrictions from cardiac and renal problems
-Humidification of the bedroom
-If no risk of choking: sucking on ice cubes or frozen juice bars
-Mash, humid food with light touch of citrus
-Rigorous dental hygiene
TO AVOID WITH XEROSTOMIC PATIENTS (SCIENCE, 2018):
-Alcohol
-Coffee
-Highly acidic food
-Sweet food
-Tobacco
TH
References
Hemalatha, V. T., Julius, A., Kumar, S. P. K., Periyasamy, T. T., & Sundar, N. M. (2019). Xerostomia: A current update for practitioners. Drug Invention Today, 12(3), 388–392. Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=a9h&AN=135900216&site=ed
Huang, Y.-C., Chu, C.-L., Ho, C.-S., Lan, S.-J., Chen, W.-Y., Liang, Y.-W., & Hsieh, Y.-P. (2015). Factors affecting institutionalized older peoples’ self-perceived dry mouth. Quality of Life Research, 24(3), 685–691. https://doi.org/10.1007/s11136-014-0792-7
James W. Little, Donald Falace, Craig Miller, Nelson L. Rhodus. (2017). Dental Management of the Medically Compromised Patient (9th Edition) [Texidium version]. Retrieved from http://texidium.com
Science, O. (2018). Google. Retrieved 06 17, 2019, from Oral Science: https://www.oralscience.com/en/protocols/xerostomia/
